
Age as a Prognostic Factor in Patients with Ewing Sarcoma—The Polish Sarcoma Group Experience

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Data Collections
2.2. Statistical Analyses
3. Results
3.1. Patients Characteristics and Treatment Outcomes
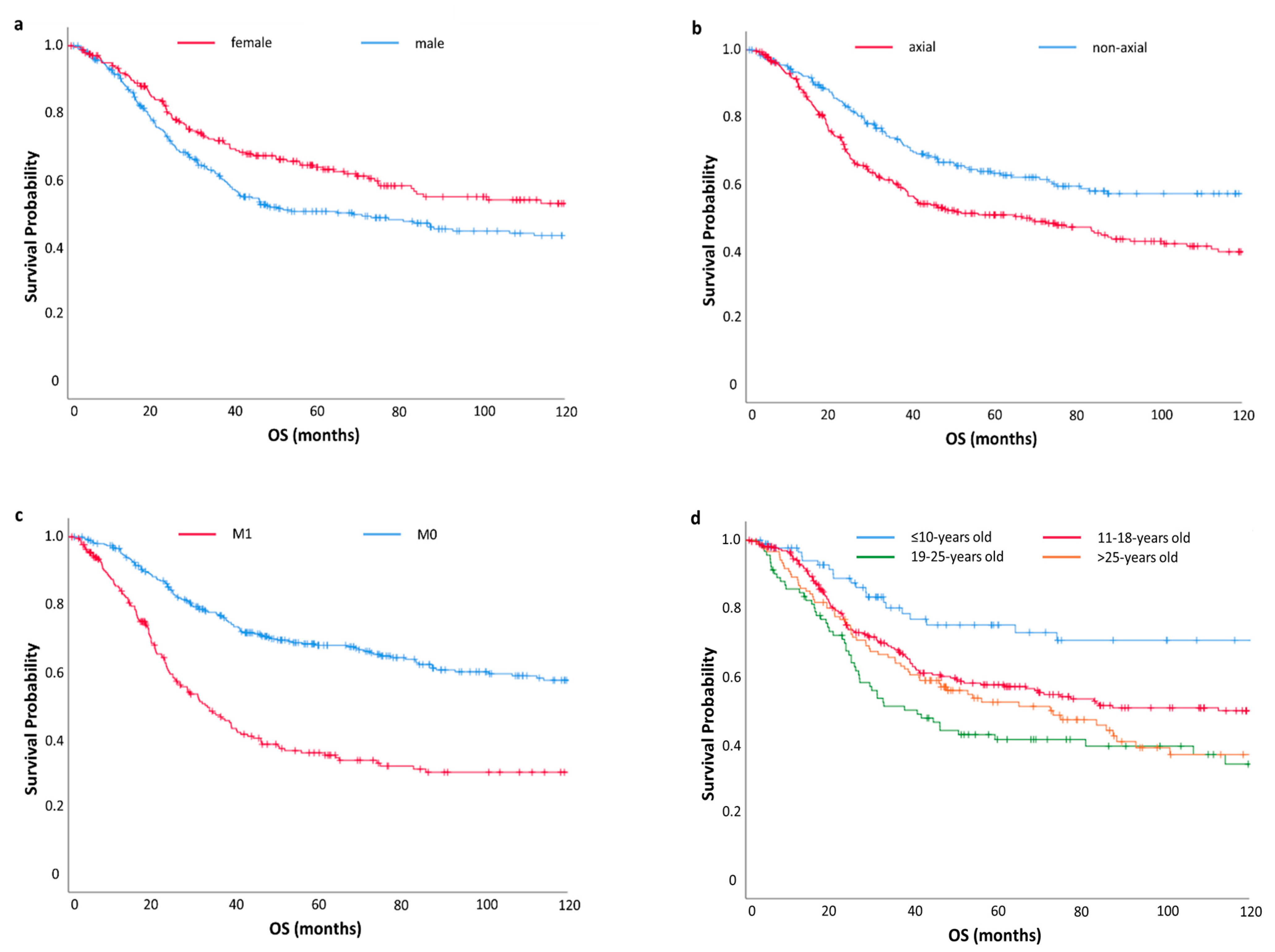
3.2. The Univariate Analysis
3.3. The Multivariate Analysis
3.4. Age Subgroups Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Casali, P.G.; Bielack, S.; Guidelines, C.P. Bone sarcomas: ESMO–PaedCan–EURACAN Clinical Practice Guidelines for diagnosis, treatment and Clinical Practice Guidelines. Ann. Oncol. 2018, 29, 79–95. [Google Scholar] [CrossRef] [PubMed]
- Tsokos, M.; Alaggio, R.D. Ewing sarcoma/peripheral primitive neuroectodermal tumor and related tumors. Pediatr. Dev. Pathol. 2012, 15, 108–126. [Google Scholar] [CrossRef]
- Cash, T.; McIlvaine, E. Comparison of Clinical Features and Outcomes in Patients with Extraskeletal Versus Skeletal Localized Ewing Sarcoma: A Report from the Children’s Oncology Group. Pediatr. Blood Cancer 2016, 63, 1771–1779. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.A.; Kim, D.H. Soft-tissue Ewing sarcoma in a low-incidence population: Comparison to skeletal Ewing sarcoma for clinical characteristics and treatment outcome. Jpn. J. Clin. Oncol. 2010, 40, 1060–1067. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damron, T.A.; Ward, W.G. Osteosarcoma, chondrosarcoma, and Ewing’s sarcoma: National cancer data base report. Clin. Orthop. Relat. Res. 2007, 459, 40–47. [Google Scholar] [CrossRef]
- Esiashvili, N.; Goodman, M. Changes in Incidence and Survival of Ewing Sarcoma Patients Over the Past 3 Decades. J. Pediatr. Hematol. Oncol. 2008, 30, 425–430. [Google Scholar] [CrossRef]
- Bosma, S.E.; Ayu, O. Prognostic factors for survival in Ewing sarcoma: A systematic review. Surg. Oncol. 2018, 27, 603–610. [Google Scholar] [CrossRef] [PubMed]
- Cotterill, S.J.; Ahrens, S. Prognostic factors in Ewing’s tumor of bone: Analysis of 975 patients from the european intergroup cooperative Ewing’s sarcoma study group. J. Clin. Oncol. 2000, 18, 3108–3114. [Google Scholar] [CrossRef]
- Bernstein, M.; Kovar, H. Ewing’ s Sarcoma Family of Tumors: Current management. Oncologist 2006, 11, 503–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, Q.T.; Teo, J.Y. A case of small bowel metastasis from spinal Ewing sarcoma causing intussusception in an adult female. World J. Surg. Oncol. 2016, 2016, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Balamuth, N.J.; Womer, R.B. Ewing’ s sarcoma. Lancet Oncol. 2010, 11, 184–192. [Google Scholar] [CrossRef]
- Duchman, K.R.; Gao, Y. Prognostic factors for survival in patients with Ewing’s sarcoma using the surveillance, epidemiology, and end results (SEER) program database. Cancer Epidemiol. 2015, 39, 189–195. [Google Scholar] [CrossRef]
- Pinkel, D. Cyclophosphamide in children with cancer. Cancer 1961, 15, 42–49. [Google Scholar] [CrossRef]
- Sutow, W.W.; Sullivan, M.P. Cyclophosphamide therapy in children with Ewing’s sarcoma. Cancer Chemother. Rep. 1962, 23, 55–60. [Google Scholar]
- Jain, S.; Kapoor, G. Chemotherapy in Ewing’s sarcoma. Indian J. Orthop. 2010, 44, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Rosen, G.; Wollner, N. Disease-free survival in children with Ewing’s sarcoma treated with radiation therapy and adjuvant four-drug sequential chemotherapy. Cancer 1974, 33, 384–393. [Google Scholar] [CrossRef]
- Worch, J.; Ranft, A. Age dependency of primary tumor sites and metastases in patients with Ewing sarcoma. Pediatr. Blood Cancer 2018, 65, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Wang, J. Clinical Features and Prognostic Factors in Elderly Ewing Sarcoma Patients. Med. Sci. Monit. 2018, 24, 9370–9375. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Huang, Y. Impact of chemotherapy cycles and intervals on outcomes of nonspinal Ewing sarcoma in adults: A real-world experience. BMC Cancer 2019, 19, 5–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.A.; Pappo, A. Clinical Outcome of Children and Adults With Localized Ewing Sarcoma. Cancer 2010, 116, 3189–3194. [Google Scholar] [CrossRef] [PubMed]
- Perisa, M.P.; Stanek, J. Evaluating Age-related Disparity of Outcomes in Ewing Sarcoma Patients Treated at a Pediatric Academic Medical Center. J. Pediatr. Hematol. Oncol. 2020, 43, 702–706. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.; Granowetter, L. Age, Tumor Characteristics, and Treatment Regimen as Event Predictors in Ewing: A Children’s Oncology Group Report. Sarcoma 2015, 2015, 927123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotz, S.J.; Nagarajan, R. Challenges in the Treatment of Sarcomas of Adolescents and Young Adults. J. Adolesc. Young Adult Oncol. 2017, 6, 406–413. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network: Bone Cancer. 2016. Available online: http://www.nccn.org/professionals/physician_gls/pdf/bone.pdf (accessed on 13 August 2021).
- Wagner, M.J.; Livingston, J.A. Chemotherapy for Bone Sarcoma in Adults. J. Oncol. Pract. 2016, 12, 208–216. [Google Scholar] [CrossRef]
- Whelan, J.; Le Deley, M.C. High-Dose Chemotherapy and Blood Autologous Stem-Cell Rescue Compared With Standard Chemotherapy in Localized High-Risk Ewing Sarcoma: Results of Euro-E.W.I.N.G.99 and Ewing-2008. J. Clin. Oncol. 2018, 36, 2516. [Google Scholar] [CrossRef] [Green Version]
- Umeda, K.; Miyamura, T. Prognostic and therapeutic factors influencing the clinical outcome of metastatic Ewing sarcoma family of tumors: A retrospective report from the Japan Ewing Sarcoma Study Group. Pediatr. Blood Cancer 2021, 68, e28844. [Google Scholar] [CrossRef] [PubMed]
- Womer, R.B.; West, D.C. Randomized Controlled Trial of Interval-Compressed Chemotherapy for the Treatment of Localized Ewing Sarcoma: A Report From the Children’ s Oncology Group. J. Clin. Oncol. 2012, 30, 703. [Google Scholar] [CrossRef] [Green Version]
- Brennan, B.; Laura, K.L. Comparison of two chemotherapy regimens in Ewing sarcoma (ES): Overall and subgroup results of the Euro Ewing 2012 randomized trial (EE2012). J. Clin. Oncol. 2020, 38 (Suppl 15), 11500. [Google Scholar] [CrossRef]
- Ries, L.A.G.; Smith, M.A. Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975–1995; National Cancer Institute, SEER Program: Bethesda, MD, USA, 1999. [Google Scholar]
- Stiller, C.A.; Passmore, S.J. Patterns of care and survival for patients aged under 40 years with bone sarcoma in Britain, 1980–1994. BMJ 2006, 94, 22–29. [Google Scholar] [CrossRef] [Green Version]
- Stachelek, G.C.; John, A. Predictors of Recurrence and Patterns of Initial Failure in Localized Ewing Sarcoma: A Contemporary 20-Year Experience. Sarcoma 2021, 2021, 6681741. [Google Scholar] [CrossRef]
- Albergo, J.I.; Gaston, C.L. Ewing’s sarcoma: Only patients with 100% of necrosis after chemotherapy should be classified as having a good response. Bone Joint J. 2016, 98, 1138–1144. [Google Scholar] [CrossRef]
- Hesla, A.C.; Papakonstantinou, A. Current Status of Management and Outcome for Patients with Ewing Sarcoma. Cancers 2021, 13, 1202. [Google Scholar] [CrossRef] [PubMed]
- Stefan, K.; Zöllner, J.F. Ewing Sarcoma—Diagnosis, Treatment, Clinical Challenges and Future Perspectives. J. Clin. Med. 2021, 10, 1685. [Google Scholar] [CrossRef]
- Sbaraglia, M.; Righi, A. Ewing sarcoma and Ewing-like tumors. Virchows Arch. 2020, 476, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, Y.; Zhang, L. The clinical heterogeneity of round cell sarcomas with EWSR1/FUS gene fusions: Impact of gene fusion type on clinical features and outcome. Genes Chromosom. Cancer 2020, 59, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Verma, V.; Denniston, K.A. A Comparison of Pediatric vs. Adult Patients with the Ewing Sarcoma Family of Tumors. Front. Oncol. 2017, 7, 82. [Google Scholar] [CrossRef] [Green Version]
- Ahn, H.K.; Uhm, J.E. Analysis of prognostic factors of pediatric-type sarcomas in adult patients. Oncology 2011, 80, 21–28. [Google Scholar] [CrossRef]
- Krakorova, D.A.; Kubackova, K. Advantages in Prognosis of Adult Patients with Ewing Sarcoma: 11-years Experiences and Current Treatment Management. Pathol. Oncol Res. 2017, 24, 623–630. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Clinicopathological Factors | Number of Patients N (%) | |
|---|---|---|
| Sex | female | 243 (43%) |
| male | 326 (57%) | |
| Age at diagnosis | ≤10 years | 91 (16%) |
| 11–18 years | 267 (47%) | |
| 19–25 years | 91 (16%) | |
| >25 years | 120 (21%) | |
| Tumor localization | axial | 322 (57%) |
| non-axial | 247 (43%) | |
| Metastases at diagnosis | M0 | 356 (63%) |
| M1 | 213 (37%) | |
| Localization of metastases | M0 | 356 (63%) |
| Lung | 97 (17%) | |
| other | 116 (20%) | |
| Pathological fracture | Yes | 31 (5%) |
| No | 533 (94%) | |
| missing data | 5 (1%) | |
| Clinicopathological factors | Number of patients N (%) | |
| Chemotherapy regimen | no CHT | 9 (2%) |
| other | 218 (38%) | |
| VIDE | 342 (60%) | |
| Local treatment | Surgery | 184 (32%) |
| RTH+surgery | 213 (38%) | |
| RTH | 116 (20%) | |
| No | 56 (10%) | |
| Type of surgery | LSS | 375 (66%) |
| amputation | 33 (6%) | |
| No | 161 (28%) | |
| Auto-BMT | Yes | 87 (15%) |
| No | 482 (85%) | |
| Disease progression | Yes | 246 (43%) |
| No | 323 (57%) | |
| Survival status | Deceased | 253 (44%) |
| Alive | 316 (56%) | |
| Chemotherapy Regimen | Age Subgroups, Number of Patients 560 (9 Patients did not Received CHT) | |||
|---|---|---|---|---|
| ≤10 Years Old (88 Patients) | 11–18 Years Old (264 Patients) | 19–25 Years Old (90 Patients) | >25 Years Old (118 Patients) | |
| EI/AC | 0 (0%) | 1 (<1%) | 34 (38%) | 50 (42%) |
| VADRIAC/EIAO | 1 (1%) | 15 (6%) | 33 (37%) | 42 (36%) |
| VIDE | 83 (95%) | 234 (89%) | 15 (17%) | 10 (8%) |
| EVAIA | 1 (1%) | 9 (3%) | 5 (5%) | 7 (6%) |
| EI | 0 (0%) | 0 (0%) | 3 (3%) | 7 (6%) |
| other | 3 (3%) | 5 (2%) | 0 (0%) | 2 (2%) |
| Prognostic Factor | 5-Year OS Rate | p-Value | |
|---|---|---|---|
| Sex | Female | 64% | 0.006 |
| Male | 51% | ||
| Age | ≤10 years old | 75% | <0.001 |
| 11–18 years old | 58% | ||
| 19–25 years old | 41% | ||
| >25 years old | 52% | ||
| Tumour location | Axial | 51% | <0.001 |
| non-axial | 63% | ||
| Metastases | M0 | 68% | <0.001 |
| M1 | 36% | ||
| Localization of metastases | M0 | 68% | <0.001 |
| Lung | 48% | ||
| Other | 24% | ||
| Pathological fracture | Yes | 49% | 0.569 |
| No | 56% | ||
| Chemotherapy regimen | no CHT | 44% | <0.001 |
| Other | 46% | ||
| VIDE | 64% | ||
| Local treatment | Surgery | 69% | <0.001 |
| RTH+Surgery | 63% | ||
| RTH | 41% | ||
| no | 19% | ||
| Type of surgery | LSS | 68% | <0.001 |
| Amputation | 46% | ||
| No | 32% | ||
| Auto-BMT | Yes | 59% | 0.198 |
| No | 56% | ||
| Variables in the Equation | p | Exp (B) | 95% CI for Exp (B) | |
|---|---|---|---|---|
| Lower | Upper | |||
| Sex: male (vs. female) | 0.002 | 1.525 | 1.170 | 1.987 |
| Tumour location: axial (vs. non-axial) | 0.005 | 1.458 | 1.120 | 1.898 |
| Metastases: M1 (vs. M0) | <0.001 | 2.641 | 2.048 | 3.407 |
| Pathological fracture | 0.290 | 1.330 | 0.784 | 2.259 |
| Age: >10y (11–18 years old, 19–25 years old and >25 years old) vs. ≤10y | 0.001 | 2.286 | 1.407 | 3.715 |
| Prognostic Factors | Age Subgroups | |||||
|---|---|---|---|---|---|---|
| <10 Years | 10–18 Years | 18–25 Years | >25 Years | p | ||
| Sex | Female | 52 (57%) | 109 (41%) | 35 (38%) | 47 (39%) | 0.024 |
| Male | 39 (43%) | 158 (59%) | 56 (62%) | 73 (61%) | ||
| Tumour location | Axial | 41 (45%) | 143 (54%) | 61 (67%) | 77 (64%) | 0.005 |
| non-axial | 50 (55%) | 124 (46%) | 30 (33%) | 43 (36%) | ||
| Metastases | M0 | 56 (62%) | 148 (55%) | 56 (61%) | 96 (80%) | <0.001 |
| M1 | 35 (38%) | 119 (45%) | 35 (39%) | 24 (20%) | ||
| Localization of metastases | M0 | 56 (62%) | 148 (55%) | 56 (61%) | 96 (80%) | <0.001 |
| Lung | 20 (22%) | 50 (19%) | 16 (18%) | 11 (9%) | ||
| Other | 15 (16%) | 69 (26%) | 19 (21%) | 13 (11%) | ||
| Pathological fracture | Yes | 5 (6%) | 17 (6%) | 2 (2%) | 7 (6%) | 0.524 |
| No | 85 (94%) | 250 (94%) | 87 (98%) | 111 (94%) | ||
| Chemotherapy regimen | no CHT | 3 (3%) | 3 (1%) | 1 (1%) | 2 (2%) | <0.001 |
| Other | 5 (6%) | 30 (11%) | 75 (82%) | 108 (90%) | ||
| VIDE | 83 (91%) | 234 (88%) | 15 (17%) | 10 (8%) | ||
| Local treatment | Surgery | 54 (59%) | 110 (41%) | 10 (11%) | 10 (8%) | <0.001 |
| RTH + surgery | 25 (27%) | 91 (34%) | 41 (45%) | 56 (47%) | ||
| RTH | 6 (7%) | 42 (16%) | 24 (26%) | 44 (37%) | ||
| No | 6 (7%) | 24 (9%) | 16 (18%) | 10 (8%) | ||
| Type of surgery | LSS | 79 (87%) | 191 (71%) | 48 (53%) | 57 (48%) | <0.001 |
| Amputation | 5 (2%) | 18 (7%) | 3 (3%) | 10 (8%) | ||
| No | 10 (11%) | 58 (22%) | 40 (44%) | 53 (44%) | ||
| Auto-BMT | Yes | 22 (24%) | 60 (22%) | 5 (5%) | 0 (0%) | <0.001 |
| No | 69 (76%) | 207 (78%) | 86 (95%) | 120 (100%) | ||
| Disease progression | Yes | 29 (32%) | 106 (40%) | 50 (55%) | 61 (51%) | 0.003 |
| No | 62 (68%) | 161 (60% | 41 (45%) | 59 (49%) | ||
| Died | Yes | 20 (22%) | 113 (42%) | 54 (59%) | 66 (55%) | <0.001 |
| No | 71 (78%) | 154 (58%) | 37 (41%) | 45 (45%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jagodzińska-Mucha, P.; Raciborska, A.; Koseła-Paterczyk, H.; Kozak, K.; Bilska, K.; Świtaj, T.; Falkowski, S.; Dawidowska, A.; Rutkowski, P.; Ługowska, I. Age as a Prognostic Factor in Patients with Ewing Sarcoma—The Polish Sarcoma Group Experience. J. Clin. Med. 2021, 10, 3627. https://doi.org/10.3390/jcm10163627
Jagodzińska-Mucha P, Raciborska A, Koseła-Paterczyk H, Kozak K, Bilska K, Świtaj T, Falkowski S, Dawidowska A, Rutkowski P, Ługowska I. Age as a Prognostic Factor in Patients with Ewing Sarcoma—The Polish Sarcoma Group Experience. Journal of Clinical Medicine. 2021; 10(16):3627. https://doi.org/10.3390/jcm10163627
Chicago/Turabian StyleJagodzińska-Mucha, Paulina, Anna Raciborska, Hanna Koseła-Paterczyk, Katarzyna Kozak, Katarzyna Bilska, Tomasz Świtaj, Sławomir Falkowski, Anna Dawidowska, Piotr Rutkowski, and Iwona Ługowska. 2021. "Age as a Prognostic Factor in Patients with Ewing Sarcoma—The Polish Sarcoma Group Experience" Journal of Clinical Medicine 10, no. 16: 3627. https://doi.org/10.3390/jcm10163627